- Categories
- Tags
ISASS Policy Statement – Lumbar Spinal Fusion
Download this Document in PDF Format >>
Contents
- Introduction
- Scope
- Definitions
- Conditions for which Lumbar Fusion is Medically indicated
- Conditions for which Lumbar Fusion is Indicated on a Case-by-Case Basis
- Conditions for which Lumbar Fusion is Not Medically Appropriate
- Scientific Background
- Conclusion
- References
Introduction
Pain and other symptoms of the lower back are some of the most prevalent health problems experienced by the populations of developed nations. They cause prolonged suffering and diminished quality-of-life to the patients, resulting in enormous losses of productivity and substantial costs for ongoing medical care. Many patients can (and should) be treated adequately by medical management, but a small portion of patients will not respond sufficiently, and some spinal conditions can never really be treated non-operatively. For these non-responders and patients with more severe spinal conditions, lumbar spinal fusion can eliminate painful motion and restore local stability and correct alignment to the spine, but proper patient selection is essential for achieving good outcomes. For decades, fusion has been the established standard surgical treatment for many conditions of the lumbar spine.
As the world continues making progress into the future, our populations are living longer lives and expecting to remain more active later into life. Medical knowledge, surgical technology, and the quality of healthcare in general have all been improving noticeably from year to year. Spine surgery in particular has undergone dramatic maturation over the past decade with many new advances in diagnostic imaging, surgical technique, and spinal implants. Furthermore, many major studies have been published just recently, providing a whole new higher level of scientific evidence to this specialty. Thus it is possible to treat many conditions and more severe patients with greater success and safety today than 20 years ago. This has led our populations to have rising expectations for medical treatment and decreasing acceptance of these painful and debilitating spinal conditions as simply an inevitable fate from ageing. At the same time, increasing success and optimism may be leading some surgeons to overuse procedures beyond what the current state of medical evidence really supports.
It has often been remarked that there is substantial geographic variation in the rates of spine surgery. Although geographic variation in treatment choices and/or insurance coverage policies can have many causes, this variation does also suggest in part a lack of collective adherence to the current state of medical evidence. Professional medical societies have the responsibility to review the evidence and provide expert guidance on the current standards of treatment. This document specifies when lumbar spinal fusion surgery is medically indicated, when it is investigational, and when it is not medically appropriate, based on the currently available scientific evidence. This Policy Statement on Lumbar Fusion thus serves to communicate clearly to all spine surgeons the indications for which our profession and the scientific evidence will or will not provide support for lumbar fusion as a medically indicated treatment.
It should be kept in mind that healthcare policy is formulated at a population-level based upon scientific evidence, some of which comes from optimally selected patient populations and carefully monitored research settings. When applied to individual patients in a routine setting, the surgeon must consider how well the evidence would apply to the individual patient. In particular, many patient factors – such as smoking, obesity, age, other medical co-morbidities, and patient psychology – may modify the outcomes that can be expected from treatment. This policy statement states which diagnoses should be eligible for lumbar fusion surgery under which general pre-conditions; the spine surgeon must still use his or her expert experience and expert judgment to determine if the individual patient is well suited for spine surgery, and if so, which specific techniques to use.
Scope
This policy statement only concerns fusion (arthrodesis); it does not concern lumbar spinal surgery in general, nor non- fusion devices or treatments. Even when suggestions are made about other forms of treatment or non-fusion surgery, they should be understood only as suggestions, beyond the scope of this policy statement.
This policy statement only applies to the lumbar spine, from T12/L1 to L5/S1.
This policy statement only applies to adult patients, 18 yrs of age and older.
This document is a Policy Statement, not a Treatment Guideline. Accordingly, it only specifies the conditions for which lumbar fusion surgery is medically indicated – i.e. which diagnoses, which patients, and after which criteria are met. This document does not provide further guidance on how a lumbar fusion should be performed (e.g. instrumented or not, procedural tips to improve outcomes, prevention of complications, etc.), nor does it discuss other treatment options. Further treatment guidance can often be found in the references cited.
Definitions
“Spondylolysis” is defined as an isthmic fracture of the pars interarticularis without vertebral slippage. Unless stated otherwise, it refers here to spondylolysis without spondylolisthesis.
“Spondylolisthesis” is defined as translational displacement or nonanatomic alignment of one vertebra relative to the adjacent vertebra. It refers here to any type of spondylolisthesis (congenital, isthmic, degenerative, traumatic, pathologic, iatrogenic).
“Stenosis” is defined as a narrowing of the spinal canal – either central, lateral, or foraminal. “Stenosis” refers here only to stenosis in the absence of other diagnoses, such as spondylolisthesis, scoliosis, etc. “Stenosis with spondylolisthesis” is covered instead under the term “spondylolisthesis”. “Stenosis with scoliosis” is covered under “scoliosis”. And so on.
“Degenerative disk disease” (DDD) refers to chronic axial low back pain presumed secondary to dehydrational and biochemical changes of the intervertebral disk, as evidenced on imaging. In this policy statement, “DDD” refers only to pure degenerative disk disease, without other codiagnoses, such as spondylolisthesis, stenosis, scoliosis, or herniated disk. When these other diagnoses co- occur, then the condition should be treated according to those other diagnoses.
“Spinal balance” refers to the alignment of the vertebrae in the standing position, viewed from anterior-posterior (AP) and lateral perspectives. The spine is normally straight from the AP view but has curves from the lateral view: lordosis at the cervical and lumbar levels and kyphosis at the thoracic levels. The spine’s sagittal alignment depends on the position of the pelvis, which is variable in a normal healthy population. An asymptomatic spine with normal alignment will require the least amount of energy to maintain posture and balance. When the spine does not have normal alignment, the body makes compensatory efforts to maintain balance and posture. This requires continuous muscle exertion which leads eventually to fatigue and pain.
Conditions for which Lumbar Fusion IS Medically Indicated
1. Emergency Situations. Lumbar fusion surgery is medically indicated in any emergency situation when the attending surgeon judges fusion to be a necessary part of surgical intervention. An “emergency situation” is any medical situation where the patient risks permanent neurological or functional deficit if he or she is not operated on emergently. Such situations may include but are not limited to: clinical signs of cauda equina syndrome or other significant neurological impairment.
2. Trauma. Lumbar fusion surgery may be medically indicated to treat some fractures or displacement of lumbar vertebrae resulting from trauma, such as motor vehicle collisions, construction accidents, vertical falls, etc.
3. Revisions. Lumbar fusion surgery may be medically indicated for some revisions at the same level of a previous surgery that show evidence of complications either causing clinical symptoms or risking harm to the patient. Such situations would include for example device failure from a previous lumbar surgery or iatrogenic instability. This indication does not included cases of mere lack of clinical improvement from an initial surgery.
4. Tumor. Lumbar fusion surgery may be medically indicated when treating primary spinal tumor, metastasis to the spine, abscess, or other growths creating a mass effect that damages or displaces the spine and/or the neural tissues.
5. Infection. Lumbar fusion surgery is often medically indicated to treat infection by any kind of foreign organism which is affecting the spine. (This includes tuberculosis.)
6. Flat-Back Syndrome. Lumbar fusion surgery, in conjunction with osteotomies, is medically indicated to correct flat-back syndrome, due to previous spinal surgery, when the patient presents with clinical symptoms or when the sagittal imbalance is progressive.
7. Pseudoarthrosis. Lumbar fusion surgery is medically indicated when all of the following conditions are met.
a. One year of time has passed since the previous lumbar fusion surgery.
b. Radiographic fusion has not been achieved, as demonstrated on dynamic radiographs or CT scans.
c. The patient presents with clinically meaningful symptoms of pain or neurological symptoms from that spinal level.
8. Adjacent Segment Degeneration. Lumbar fusion surgery is medically indicated when all of the following conditions have been met.
a. The patient has previously undergone fusion (for any diagnosis), which at some point resulted in substantial clinical improvement for a period of at least 6 months.
b. Imaging shows clear signs of disk degeneration, instability, and/or stenosis, at a level immediately adjacent to the fusion, which either were not present at the time of the original operation or have worsened from their initial state an amount that is clinically substantial.
c. The patient presents with clinically meaningful pain or neurological symptoms, which have been unresponsive to a minimum of 3 consecutive months of structured conservative medical management (including at least pain medication, activity modification, and daily exercise).
9. Deformity. Lumbar fusion surgery is medically indicated for deformity (e.g. scoliosis) when all of the following conditions have been met.
a. Painful and/or progressive deformity in the sagittal and/or coronal planes with evidence of disability and loss of function. Patients who are most symptomatic usually show radiographic evidence of:
i. global malalignment in the sagittal plane as determined by the C7 plumbline,
ii. loss of lumbar lordosis as judged by pelvic tilt,
iii. spondylolisthesis, lateral listhesis, retrolisthesis, or combinations thereof.
b. The patient has not shown adequate clinical improvement from a minimum of 3 consecutive months of conservative medical management (including at least pain medication and muscle strengthening exercise). c. The patient has been explicitly interviewed about possible unexpressed cosmetic concerns, and (if present) the patient has been properly and realistically informed about the effects of surgery on postural appearance and the recovery process involved.
10. Spondylolisthesis. Lumbar fusion surgery is medically indicated for any type of spondylolisthesis when all of the following conditions are met.
a. The patient has clinically important pain or neurological symptoms.
b. The patient has not shown sufficient clinical improvement from at least 3 months of conservative care.
11. Spondylolysis. Lumbar fusion surgery is medically indicated when all of the following criteria are met.
a. The patient presents with meaningful levels of pain in the back and legs.
b. Spondylolysis has been radiographically documented in an anatomic area consistent with the location of these symptoms, whereby lysis blocks may be useful to correlate symptoms with the imaging.
c. The patient has failed to improve from a minimum of six months of conservative medical management.
12. Recurrent Disk Herniation. Lumbar spinal fusion surgery is medically indicated for recurrent disk herniation, when all of the following conditions are met:
a. The patient has previously been operated at the same level for disk herniation, which resulted in meaningful symptom relief for at least 3 months.
b. Recurrent disk herniation is seen on imaging at the same level that was previously operated.
c. The patient has new pain or neurological symptoms consistent with the level of recurrence.
d. The patient either has acute neurological symptoms that cannot wait longer for surgical treatment or has been unresponsive to 3 months of conservative medical management (including at least pain mediation and exercise).
13. Stenosis with Instability Documented Pre-Operatively or Intraoperatively. When performing decompression for spinal stenosis, fusion surgery is medically indicated if either one of the following two conditions is met:
a. The patient had pre-operative instability demonstrated on dynamic imaging.
b. Spinal instability has arisen intraoperatively because adequate decompression required creation of a pars defect or removal of either 75% of one facet joint or 50+% of both facet joints.
14. Degenerative Disk Disease (DDD). Lumbar spinal fusion surgery is medically indicated – at a maximum of two levels – when all of the following conditions are met.
a. The patient presents with clinically important pain and disability consistent with diskogenic pain.
b. MRI (or other imaging) demonstrates morphological disk degeneration.
c. The patient has not shown sufficient improvement from a minimum of 6 consecutive months of structured conservative medical management (including at least pain medication, activity modification, and daily exercise), with adequate patient compliance.
d. The patient has then subsequently not shown sufficient improvement from a program of intensive multidisciplinary rehabilitation, (with a minimum volume of 80 hours of on-site treatment during a 2-4 week period, including a cognitive- behavioral component), if such a program is locally available and covered by the patient’s insurance.
e. The patient has been appropriately screened for possible mental illness and/or substance abuse issues, and if present has undergone professional treatment for these issues.
f. The patient is not currently involved in an ongoing litigation case related to his or her back. (This does not refer to “worker’s compensation”.)
g. The patient is age 25-65.
h. The patient is not pregnant.
i. Either provocative discography (with concordant pain and negative adjacent levels) or magnetic resonance spectroscopy (MRS) has provided corroborating evidence that the patient’s pain is likely due to the disk degeneration observed on imaging, and the two are not merely an unrelated coincidence.
Conditions for which Fusion is Indicated on a Case-by-Case Basis
15. Rare and Unusual Cases. Lumbar fusion surgery is investigational but medically appropriate for rare and unusual cases. Lumbar fusion surgery may be considered and receive healthcare coverage when all of the following conditions have been met.
a. The patient’s condition is not addressed by any of the situations discussed elsewhere in this document.
b. The treating surgeon has reviewed the case with at least two other spine surgeons at different institutions.
c. The treating surgeon has asked the patient if he or she would consent to anonymous publication of his or her case history in a scientific journal, and if the patient has consented, the treating surgeon has committed himself or herself to publishing a case report on this rare patient and his or her surgical treatment.
16. Degenerative Disk Disease in the Elderly. Lumbar fusion surgery for pure DDD without other co-diagnoses is rare in patients over age 65 and has been poorly studied. Nonetheless, it may be considered an appropriate standard of care in select cases. Lumbar fusion surgery – at a single level – is medically appropriate for elderly patients who meet all the conditions listed above for patients age 25-65.
17. Degenerative Disk Disease at Multiple Levels. Lumbar fusion surgery at 3 or more levels for pure DDD in the absence of other co-diagnoses is considered investigational and is not normally performed in a routine setting. Likewise, lumbar fusion surgery at 2 levels in patients over age 65 for pure DDD in the absence of other co-diagnoses is not normally performed.
18. Facet Syndrome. Lumbar fusion surgery for facet syndrome is no longer commonly supported and should only be performed in the context of a prospective clinical research study.
Conditions in which Lumbar Fusion is NOT Medically Appropriate
19. Pure Stenosis (without any of the other diagnoses mentioned above).
20. Initial Disk Herniation (in the absence of any other diagnosis mentioned above).
21. Chronic Low Back Pain without Any Clear Cause on Imaging.
Scientific Background
This Policy Statement limits itself to providing the medical rationale and scientific evidence for indications which have not yet already achieved widespread consensus.
1. Emergency Situations.
2. Trauma.
3. Revisions.
4. Tumor.
5. Infection.
6. Flat-Back Syndrome.
Flat-back syndrome as defined in the literature refers to the iatrogenic loss of lumbar lordosis, accompanied by back pain, forward inclination of the trunk, and inability to stand erect.[Farcy; Lagrone; Wiggins] The patient may experience pain not only in the lower back but also at thoracic and cervical levels, in the hips, thighs, knees, and neck, all as a result of muscle fatigue from trying to compensate for loss of sagittal balance. Physical therapy and/or mere removal of pre-existing instrumentation may provide adequate pain relief in some patients, at least in the short-term.[Farcy] Further surgical treatment is indicated if the patient remains symptomatic or if the sagittal imbalance is progressive. The goal of treatment is restoration of sagittal balance, which should relieve the patient’s pain. Osteotomies are the main approach to surgical treatment, but fusion may also be needed at some levels to restabilize the spine in the correct anatomical position, depending on the specifics of the case.
Patients with loss of lumbar lordosis but no history of past spine surgery are not included under this indication. They should be assessed as a “Deformity” patient under point # 9.
The correct standing position is characterized by a straight spine on the AP view and curvature on the sagittal view. This allows a person to maintain equilibrium and a horizontal gaze. This normal balance also economizes the amount of energy spent through muscles to maintain posture or locomotion. In the sagittal plane, the shape of the spine is quite variable in the normal population, and there is a strong relationship between the shape of the spine and the position of the pelvis.[Legaye; Roussouly] Since the position of the pelvis is essentially fixed, all modifications of the shape of the spine (due to ageing or otherwise) lead to compensatory phenomena. Ageing for example, often leads to kyphosis, due to disk degeneration and loss of disk height. Spine imbalance is intrinsically linked with the aging process, but can arise from surgery as well.
Patients with spine imbalance should be considered even for a single-level pathology. Imbalance is not related only to previous surgery or what is traditionally termed “deformity” (i.e. important scoliosis or kyphosis with Cobb angle higher that 30 or 40 degrees). Imbalance can also occur with a simple single-level spondylolisthesis or DDD. Imbalance can be measured with high accuracy using full-spine, lateral, standing X-rays, and well-known parameters can be calculated.[Legaye; Roussouly] The pelvic parameters are crucial to analyze before any kind of fusion surgery, in order to avoid postoperative misalignment. Postoperative sagittal malalignment can lead to inadequate fixation, flatback syndrome, and/or adjacent segment degeneration, due to inappropriate load transmission and overstress. Thus, sagittal balance must be maintained in any kind of lumbar fusion.[LeHuec] Sagittal imbalance after lumbar fusion is highly correlated with poor clinical outcomes. Sagittal balance maintenance or restoration does not change the surgical procedure for lumbar fusion. It is only a parameter to analyze before the surgery in order to restore the appropriate spine contour by lordosis restoration.
References: Bourghli; Farcy; Lagrone; Legaye; LeHuec; Mac-Thiong; Pellet; Roussouly; Wiggins
7. Pseudoarthrosis. Lumbar fusion surgery aims to achieve its clinical treatment goals by eliminating motion and providing stability at the operated level. Sometimes the clinical treatment goals are achieved despite a lack of radiographic fusion and presence of substantial range of motion at the operated level. When the clinical goals are achieved, further surgery is generally not warranted, even if pseudoarthrosis is present. If the clinical goals have not been achieved, and pseudoarthrosis is clearly shown on radiographic imaging taken at least one year after the initial surgery, then repeat surgery is normally warranted, because the initial surgery has not been biotechnically successful and therefore did not have sufficient capability to be clinically successful.
It is been shown repeatedly that smoking is a substantial risk factor for pseudoarthrosis,[Andersen; Brown; Lee] possibly because nicotine inhibits early revascularization of the bone graft.[Daftari] Thus, patients who smoke are counteracting the mechanism of action of fusion surgery and undermining their chances for a successful outcome. If a patient has already had a fusion surgery which was unsuccessful because of pseudoarthrosis, then steps should be taken to avoid a repeat failure. This often includes cessation of smoking and interbody fusion techniques to improve fusion rates.
References: Andersen; Brown; Daftari; Lee; Sherman
8. Adjacent Segment Degeneration.
Adjacent segment degeneration (ASD) is defined as symptomatic degenerative changes (including stenosis, spondylolisthesis, or herniated disc) at a level adjacent to a previous fusion. The etiology is multifactorial, and degenerative changes may in part reflect “natural” disease progression. Nonetheless, ASD can be viewed as a late complication of fusion, resulting in part from the loss of segmental motion at the originally fused level. If the original fusion was clinically beneficial for a time, then extending it to the ASD level should also be beneficial. The fusion should only be extended to the ASD level if the original fusion resulted in meaningful clinical improvement for a period of time. If the original fusion was never beneficial, then extending it will probably not result in clinical improvement either.
The patient should present with clinically meaningful symptoms that do not respond to conservative medical management. Conservative care should be tried first, because patient complaints of pain may have causes other than the degeneration seen on imaging and may be responsive to conservative care. Asymptomatic degeneration can often be found on imaging, but is not an indication for surgery.
References: Levin; Park
9. Deformity. “Deformity” refers here all-inclusively to any malalignment of the spine, regardless of which planes the malalignment occurs in or what the etiological causes are. Regrettably, health policy for adult deformity has often become confused by reviewing the medical literature on adolescents. When deformity occurs in adolescents who are still growing, the goal of treatment is usually to prevent further curve progression and the later health consequences that progression would entail. But when deformity is diagnosed in an adult, this concern about patient growth driving further progression is not applicable.[Angevine; Berven 2007; Birknes] Therefore, the decision for surgery should instead be based upon the patient’s current condition – i.e. their clinical symptoms and magnitude of deformity. The main goal of treatment in the adult is to relieve the pain or other symptoms that the patient already has. As stated in the “Scope” section, this Policy Statement does not apply to patients that have not yet reached skeletal maturity.
Although the deformity’s etiology – degenerative, congenital, neuromuscular, idiopathic, traumatic, iatrogenic – plays a role in the evaluation and treatment of adult deformity patients, the indications for lumbar fusion surgery at a policy level come down to the same basic criteria: a) curve magnitude or progression, b) symptoms, c) disability, d) non-responsiveness to conservative care, and e) and proper patient counseling. Thus this policy statement does not differentiate by etiology, even though the details of treatment may depend on the etiology.
Deformity is a complex spinal condition. Treatment decision-making and planning is an intricate process that must take numerous factors into consideration.[Aebi; Schwab 2010] So it should be emphasized here that this document is only a policy statement; this is not a treatment guideline discussing everything the surgeon should take into consideration. This document merely outlines the criteria for when lumbar fusion surgery would be medically appropriate to treat adult deformity.
In some cases it may be possible to provide relief of radicular pain or deficit in deformity patients without fusion.[Aebi, Herkowitz; Silva] But this is the exception rather than the rule and may involve a small decompression of a unilateral mononeuropathy. The decision on whether or not to fuse depends on numerous details of the specific case, which only an extensive treatment guideline could begin to address.[Schwab 2006; Silva] If the patient meets the criteria listed here, then lumbar fusion should be considered medically indicated.
The patient should present with symptoms that diminish function.[Aebi] Surgical treatment of asymptomatic deformity in skeletally mature adults is not warranted and is not a judicious use of finite healthcare resources. Symptomatic patients should undergo conservative medical management first, since symptoms such as back pain occur commonly in the general population as well and often can be adequately treated conservatively[Lonstein] Bracing is not usually appropriate in adult patients. [Angevine; Silva]
Cosmetic concerns may be part of the motivation of adult deformity patients to seek surgery.[Lonstein; Oskouian] But patients often may not clearly express this treatment agenda. Cosmetic concerns may substantially skew the patient’s treatment decisions, especially if the patient suffers from low self-esteem, distorted body image, social withdrawal, or depression. Surgeons should explicitly ask patients about possible cosmetic motivations, and if present should carefully counsel the patient. Patients may be poorly informed about the duration and rigors of post-operative recovery. Also, patients with cosmetic motivations may have unrealistic expectations about the amount or nature of surgical correction, leading to disappointment even with excellent clinical outcomes. In order to assure proper patient selection and satisfaction, it is important to explore these issues explicitly with the patient.References: Aebi; Angevine; Berven 2007; Birknes; Herkowitz; Lonstein; Oskouian; Pritchett; Silva; Schwab 2006; Schwab 2010.
10. Spondylolisthesis.
Several high-quality studies provide more than adequate evidence that surgery provides better clinical outcomes for spondylolisthesis than conservative care and that fusion provides better outcomes than decompression alone. The procedure also has an acceptable safety profile. The type of spondylolisthesis should not play a role in treatment decisions; the condition is essentially the same regardless of etiology and similar outcomes can be expected. Similarly, neither the radiographic grade of slippage nor its progression plays a decisive role in treatment decision. The severity of the clinical status (pain or neurological symptoms) is what determines the type of treatment. Spondylolisthesis should be treated when symptomatic and unresponsive to conservative care.
References: Berven 2009; Jacobs; Martin; Metz; Resnick pt 9; Sansur
11. Spondylolysis without Spondylolisthesis.
When spondylolysis occurs together with spondylolisthesis, then it is treated according to point #10 above. Symptomatic spondylolysis without spondylolisthesis occurs most commonly in adolescent athletes, who are outside the scope of this policy statement on adults. When symptomatic spondylolysis occurs in adults, structured conservative care should be tried first for a minimum of 6 months to a year. In the vast majority of cases, pain presumably from spondylolysis can be treated sufficiently by conservative medical management. If conservative care fails, fusion might be considered a treatment option. Spondylolysis without spondylolisthesis is unlikely to be of new onset in an adult patient and therefore is also not likely to be the cause of clinical symptoms.[Brooks; Kalichman] For this reason, it is advised that lysis blocks be used to determine whether the patient’s symptoms correlate with the spondylolysis observed on imaging. There appears to be only few studies available about surgical treatment of spondylolysis without spondylolisthesis.
References: Brooks; Kalichman; Klein; Kurd; Lim
12. Recurrent Disk Herniation. Reviews of the evidence have recommended fusion as medically indicated treatment for same- level recurrent disk herniation.[Herkowitz; Resnick pt 8; Swartz]
Diskectomy and/or decompression without fusion are also plausible treatment options for recurrent disk herniation (especially with pure leg pain and minimal to no back pain), but they have a higher risk for needing further surgery. A large population-based study reported that patients who underwent surgery for a recurrent disk herniation had a 25% risk of additional surgery within the following 10 years.[Österman] This risk was reduced substantially if the initial reoperation was a fusion. Thus fusion for recurrent disk herniation is a much more definitive procedure that reduces the risk of needing further surgery, though it currently remains unclear if this is due to superior clinical outcomes or surgeon reluctance to operate further on a level that has already been fused. The decision to have fusion or some other form of surgery for recurrent disk-herniation should be shared by the patient and surgeon.
References: Herkowitz; Österman; Resnick pt 8, Swartz
13. Stenosis with Intraoperatively Documented Instability.
Review papers have recommended fusion as a treatment option in addition to decompression in patients with lumbar stenosis with evidence of spinal instability. Spinal instability may have been present pre-operatively and/or may arise or increase intraoperatively as an unavoidable result of a decompression procedure. Surgeons should plan such operations carefully and try to achieve adequate decompression without increasing instability, if possible. Nonetheless, the main goal of surgery for stenosis is the decompression, and achieving this goal will sometimes unavoidably lead to spinal instability.
The choice of whether or not to perform a fusion in these patients relies upon the clinical judgment of the surgeon at the time of operation, but fusion is generally preferred when instability is present. Many stenosis patients with intraoperative iatrogenic spinal instability who do not receive fusion must return for subsequent surgery that could have been avoided by performing a fusion. Even if seen pre-operatively, spinal instability should be assessed intraoperatively. If there has been violation of the pars interarticularis or the facet joints have been resected more than 75% unilaterially of 50% bilaterally, then the patient is better served by adding a fusion.
(According to the definitions used here, stenosis patients with spondylolisthesis are treated as spondylolisthesis patients under point #10. Stenosis patients without any co-diagnosis and without intraoperatively documented instability are treated under point #19.)
References: Herkowitz; Hopp; Knaub; Resnick pt 10; Sengupta
14. Degenerative Disk Disease (DDD).
During the past decade, there has been extensive controversy about whether fusion is beneficial for lumbar DDD. During these years, high-quality evidence has gradually accumulated to provide answers, and discussion in the medical community has led to many specific insights about the issues involved. At the present time, there is now a sufficient body of high-quality scientific evidence upon which to base treatment and policy decisions.
The most recent review paper [Coe] included six rigorously conducted, randomized comparative trials on fusion at 1 or 2 levels for pure DDD. They concluded that “fusion appears superior to unstructured nonoperative treatment, similar to structured nonoperative treatment, and similar to short-term results of artificial disc replacement”. A few months earlier, the American Pain Society reviewed the same 4 of these 6 trials that compared fusion to non-operative treatment.[Chou 2009b], and they came to much the same conclusion. The Evidence-Based Clinical Practice Guidelines from the American Pain Society gave a “grade B” recommendation to fusion surgery for nonradicular low back pain with common degenerative changes.[Chou 2009a] A grade B recommendation is one in which, “The panel recommends that clinicians consider offering the intervention to eligible patients. The panel found at least fair evidence that the intervention improves health outcomes and concludes that the benefits moderately outweigh harms”.[Chou 2009a] Interdisciplinary rehabilitation was the only other intervention to receive a grade B recommendation, and no other form of treatment received a grade A or even C recommendation. (Artificial disc replacement received grade B for outcomes to 2-years and grade I for long-term outcomes.) Key outcomes for the fusion group in these 6 randomized comparative trials are summarized in the following table.
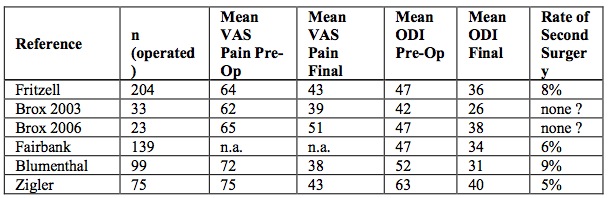
Assessing these results, it can be seen that lumbar fusion surgery is efficacious on average. The mean reduction in back pain is clinically substantial in most studies. The mean improvement in functioning (ODI) usually meets the minimum clinically important difference. And the rate of further surgery in the short-term appears acceptably low.
Since those two recent systematic reviews were conducted, 3 of these 6 trials have published further mid-term outcomes. Brox and colleagues combined their two earlier randomized controlled trials [Brox 2003; Brox 2006] and reported the combined 4- year outcomes.[Brox 2010] Consistent with the 1-year reports, mean VAS back pain in the fusion group decreased from 63 at pre- op to 41 at 4-years, and mean ODI decreased from 44 at pre-op to 29 at 4-years. By 4 years, 25% of fusion patients had undergone re-operation. Similarly, the Charité FDA IDE trial has now published 5-year outcomes on 43 ALIF control patients and reported an overall FDA-defined success rate of 51%,[Guyer] which is consistent with the 2-year outcomes reviewed by Coe and colleagues.[Coe] At 5 years, the fusion group had 47% full-time employment, 16% additional index-level surgery, and 72% patient satisfaction.[Guyer] But this report is limited by the fact that half the original sample was either de-approved or lost to 5-year follow-up, and the method of fusion used – BAK cages with iliac crest bone graft – has been “largely abandoned”.
Furthermore, two other papers have reported on fusion data for pure DDD from randomized comparative trials on arthroplasty. First, the Pro-Disc FDA IDE trial has just published the two-year outcomes on 2-level circumferential fusion patients.[Delamarter] This study is a high-quality prospective randomized multicenter comparative trial. There were 32 of 67 fusion patients who met a lengthy 10-point FDA composite definition of success. Mean VAS pain score dropped from 75 at pre-op to 38 at 2-years, which is a clinically substantial average improvement, yet the proportion of narcotics users only decreased from 46/72 at pre-op to 35/59 at 2-years. A minimum 15 point improvement on ODI was seen in 60% of the fusion patients, and at the 2-year follow-up 62% of the fusion patients said that they would have the same surgery again. Second, a prospective randomized comparative trial on arthroplasty assigned 72 adult pure DDD patients to PLF or PLIF at 1 or 2 levels.[Berg] Mean VAS back pain decreased from 59 at pre-op to 29 at 2-years, while ODI decreased from 41 to 23. There were 6 major complications and 7 further surgeries plus 20 patients having instrumentation removed for “screw irritation”. At 2-years, 76% of fusion patients were back to work part or full time and 67% were satisfied with their surgery. This study shows that good clinical outcomes can be achieved in the majority of patients, yet the rate of further surgery is not negligible.
Also since those two recent systematic reviews, two more prospective multicenter studies (conducted for the US FDA) on fusion for pure DDD have been published. First, a recent paper reported the 6-year follow-up of an FDA Phase IV study, combining patients from most sites of two previous FDA IDE trials on ALIF (LT-Cage with INFUSE rhBMP-2) for patients with DDD (and possibly grade I spondylolisthesis) not responding to conservative care.[Burkus] This study reported a combined mean ODI of 52 at pre-op, 20 at 1-year and 21 at 6-years, which represents a substantial improvement in daily functioning, with 79% of patients attaining the MCID of 15 points on ODI. Second, a multicenter prospective randomized comparative trial on ALIF for single-level DDD (and possibly grade I spondylolisthesis) randomized 78 patients to cylindrical threaded titanium cages and 62 to femoral ring allografts, both with autogenous iliac crest bone graft.[Sasso 2004] Mean ODI was reduced from 51 at pre-op to 30 at 2-years in the cylindrical titanium cage group and was virtually identical in the femoral ring allograft group. Second surgery was required in 28% of the cage group and 50% of the ring group.
Additionally, the Swedish National Spine Registry reported one-year outcomes for 671 DDD patients, 94% of whom received some kind of fusion.[Strömqvist] Mean back pain improved from 63 to 34, and 72% of patients were satisfied with the outcome of surgery. It is not clear what proportion of these patients had pure DDD without any other co-diagnoses, but the results from this large registry provide solid evidence that good clinical outcomes can be achieved in routine clinical settings for a large majority of DDD patients.
Finally, a metaanalysis covered all publications on non-revision fusion for lumbar degenerative diseases during a 20 year period, apparently regardless of study design or size, so long as the number of patients by diagnosis was clearly reported.[Bono] They pooled the results for 2226 patients treated by fusion for DDD (without disc herniation, spondylolisthesis, or scoliosis, and not specified whether stable or unstable). They found that good or excellent clinical outcomes were achieved in 73% of these patients. The complication rate was 7%. A major limitation of this metaanalysis is that 10 of 78 original studies did not report complication rates and 19 of 78 did not report clinical outcomes, but the metaanalysis left it unclear how many of the 2226 patients were therefore lacking such data and made no attempt to account for how this missing data may have skewed the remaining results. Nonetheless, this metaanalysis provides a crucial quantitative synthesis of 20 years worth of published evidence on fusion for pure DDD.
So altogether, there is a large body of high-quality scientific literature on fusion for lumbar DDD: two systematic reviews on 6 randomized comparative trials, two further reports of mid-term outcomes from 3 of these trials, two other randomized comparative trials against arthroplasty, two other high-quality prospective multicenter studies, a national patient registry, and a metaanalysis of 20 years worth of other research reports. Today, it is impossible to claim that there is insufficient evidence about lumbar fusion for DDD to make treatment or policy decisions.
On the whole, the body of scientific evidence consistently supports the use of fusion for lumbar DDD. However, the available research and further scientific discussion have also made it clear that the question of whether or not fusion should be used for lumbar DDD is far from having a simple “Yes or No” answer for all cases, as it does in most other diagnoses. Patient selection and the treatment algorithm require careful consideration of numerous details and secondary findings from the research literature, of which most people do not have a clear and comprehensive overview. So in an indication as complex as DDD, professional societies must step in and provide structure, limits, and guidance to the treatment choices of individual surgeons and their patients. Proper patient selection and the optimal treatment choice algorithm for lumbar DDD are complex issues that cannot simply be left to the personal preferences and gut instincts of individual surgeons and patients. These choices must be guided by society’s consensual collective understanding of the available medical evidence, in order to ensure that finite healthcare resources are channeled to the appropriate recipients at the appropriate time.
Therefore, the patient should exhaust appropriate non-surgical treatment options before being evaluated for surgery. The first stage is a minimum of 6 consecutive months of structured conservative medical management. The content of such medical management should be decided by the treating physician, but typically includes at least pain medication, activity modification, and daily exercise. During this period of conservative care, smokers should be strongly encouraged to stop smoking, and obese patients should be encouraged to lose weight, as smoking and obesity aggravate low back pain, are risk factors for multiple systemic health problems, and will increase the risk of poor outcomes from spine surgery.[Alkherayf; Das; Deyo; Fairbank; Heuch; Leboeuf-Yde; Lee; Lyznicki; McIvor; Møller; Nejat; Patel; Shamji; Sherman; Smith; Sutherland; Vogt; Warner; Woolf; Zimmermann-Stenzel] Further, it cannot simply be assumed that patients will adhere adequately to this treatment regime by themselves. In fact there is good reason and evidence to assume that many patients with chronic conditions are non-compliant with their prescribed treatment.[Broekmans; Evans; Jack; Wahl; Wright] Therefore, patients should be seen frequently to monitor their adherence, adjust their treatment, and document their clinical progress.[Bloom; Gold; Kornbluth; Rosenow] Otherwise, the stipulation that patients undertake 6 months of conservative care may be little more than a meaningless waiting period.
If this 6 months of conservative medical management does not result in adequate clinical improvement, then the next step in the treatment algorithm would be a program of intensive multidisciplinary rehabilitation (IMR), if such a program is available in the patient’s local area and covered by their health insurance. Three high quality randomized controlled trials comparing IMR to fusion surgery for lumbar DDD have all shown that IMR can achieve clinical outcomes equivalent to fusion surgery.[Brox 2003; Brox 2006; Brox 2010; Fairbank] Two systematic reviews have therefore recommended IMR as an equivalent treatment option, which however has none of the risks of surgery.[Coe; Chou 2009b] If IMR is available and covered by the patient’s insurance, there is no reason why a patient should not first try IMR. If IMR does not provide adequate clinical benefit, then fusion surgery still remains an available treatment option afterwards. Specifying the content of an IMR program is beyond the scope of this policy statement, but based on the literature,[Brox 2003; Fairbank; Guzmán] such a program should consist of a minimum volume of 80 hours of on-site treatment during a 2-4 week period, and should include a prominent cognitive-behavioral component, not merely physical therapy alone.
The next step is to screen the patient for possible mental illness and/or substance abuse issues. It is known that there is a high incidence of psychiatric co-morbidity (depression, anxiety, psychosomatic disorders) and substance abuse (narcotics or other drugs) among DDD patients, and it is known that these patients often have worse clinical outcomes.[DeBerard; LaCaille 2005] The screening should be done by professionals with experience in these area, as these issue are often not apparent to treating physicians and surgeons in the course of routine patient contact.[Daubs; Goldman; Gonzales; Lemelin] If psychiatric co-morbidity or substance abuse issues are identified, they should be treated before assessing the patient further for lumbar surgery, unless it can be established that these issues are a direct consequence of the back pain and disability for the specific patient.
DDD patients involved in ongoing litigation should be deferred until after the conclusion of their court case. They are very poor candidate for surgery, and several studies have reported that patients in litigation have less clinical improvement from surgery.[DeBerard; Fritzell; LaCaille 2007; LaCaille 2005] Indeed, many of these patients may be seeking surgery primarily to provide further evidence in court that they have been permanently injured.[DeBerard; Florence]
The recommendation for lumbar fusion surgery for DDD is based primarily upon 6 high-quality randomized comparative trials.[Coe] These 6 studies included patients in the following age ranges: 25-65, 18-55, 25-60, 25-60, 18-60, 18-60. Patients outside these age ranges were excluded by protocol. It cannot be automatically assumed that the results obtained in these studies would apply equally to patients outside these age ranges.[Schafer] Thus, patients over age 65 are dealt with separately, under indication #16 below. It would be rather unusual to find DDD in a patient under age 25. Such patients should be re-evaluated and/or treated conservatively until reaching 25. They might also be considered under indication #15, to understand better why symptomatic disk degeneration would occur at such a young age.
Women who are pregnant should wait until after the birth of their child to be considered for fusion surgery for DDD. Elective surgery of any kind represents an unnecessary risk to the fetus. Three of the six randomized comparative trials that serve as the basis for recommending lumbar fusion for DDD excluded pregnant women, and it is improbable that the other 3 trials actually enrolled any pregnant women.[Coe] Backache is common during pregnancy but has no particular relation to DDD.[Powell]
As a final step, candidates for lumbar fusion surgery should undergo provocative discography, in order to establish a connection between the disk degeneration seen on imaging and the back pain reported by the patient. Although disk degeneration is not a “normal” part of ageing, it does frequently occur as people grow older.[Adams; Haefeli; Miller; Powell] Disks that appear degenerated on imaging are often found in asymptomatic persons.[Adams; Boos; Powell; Urban] So when degenerated disks are painful, the pain is probably not due to the macroscopic morphological degeneration seen on the imaging but instead to biochemical or microanatomical changes that are occurring within the degenerated disk.[Haefeil] These biochemical and/or microanatomical changes only occur in disks that are morphologically degenerated, but they do not occur in all or even most disks that are degenerated.[Adams; Urban] At the same time, low back pain can have many other causal factors besides disk degeneration. Therefore it should not be assumed that the patient’s reported subjective back pain is necessarily due to the disk degeneration seen on imaging – the two may sometimes be an unrelated coincidence. So there is a need for some further diagnostic test to rule out coincidences and establish a linkage between the disk degeneration seen on imaging and the pain reported by the patient. Traditionally, this diagnostic test has been provocative discography. Although diskography has become somewhat controversial,[Carragee 2009] there is not yet any established better way to rule out the occurrence of unrelated coincidental disk degeneration in chronic low back pain patients. When used carefully, at this last patient selection step before surgery, diskography is a sensible way to verify that the patient’s pain is due to the disk degeneration, and reduce the risk of performing a fusion on a patient who predictably will not benefit from it, because their intervertebral disk is not the source of their pain, despite the appearance of degeneration on imaging. But diskography should not be used as the only indicator for surgery. Overuse will result in excessive surgeries with low success rates. The use of diskography should be reserved for well-selected candidates for fusion whose symptoms are consistent with diskogenic pain. The diskography should serve to attempt to isolate the patient’s pain generator. The emerging diagnostic test of magnetic resonance spectroscopy (MRS) may provide a promising alternative to provocative diskography that does not require any additional procedures on the patients beyond the MRIs they would already have anyway. Chemical assays of disk biopsies for inflammatory cytokines such as TNF-α may in the future be another alternative to provocative diskography. In the meanwhile, provocative diskography remains a widely used test to verify the connection between degeneration seen objectively on imaging and the patient’s reports of subjectively experienced pain. Provocative diskography should improve the rate of successful lumbar fusion, by filtering out patients in whom disk degeneration and chronic low back pain are an unrelated coincidence.[Borthakur; Cohen; Colhoun; Errico; Resnick pt 6; Tsang] In patients with degeneration at multiple levels, these tests may also help the surgeon to select the right one or two levels to fuse.
Several high-quality clinical trials have demonstrated that lumbar fusion surgery provides meaningful clinical improvement to a majority of DDD patients. Using the patient selection criteria and treatment algorithm presented here, good clinical outcomes should be expected in most patients treated.
References: Adams; Alkherayf; Andersen; Berg; Bloom; Blumenthal; Bono; Boos; Bortakur; Broekmans; Brown; Brox 2003; Brox 2006; Brox 2010; Burkus; Carragee 2009; Chou 2009b; Chou 2009a; Coe; Cohen; Colhoun; Das; Daubs; DeBerard; Delamarter; Deyo; Errico; Evans; Fairbank; Florence; Fritzell; Gold; Goldman; Gonzales; Guyer; Guzmán; Haefeli; Herkowitz; Heuch; Jack; Kornbluth; LaCaille 2007; LaCaille 2005; Leboeuf-Yde; Lee; Lemelin; Lyznicki; McIvor; Miller; Møller; Nejat; Patel; Powell; Resnick pt 6; Rosenow; Sasso 2008; Sasso 2004; Schafer; Shamji; Sherman; Smith; Strömqvist; Sutherland; Tsang; Urban; Vogt; Wahl; Warner; Woolf; Wright; Zigler; Zimmermann-Stenzel
15. Rare and Unusual Cases.
In the course of their careers, many spine surgeons will occasionally come across patients whose condition does not fit clearly into any of the diagnostic categories foreseen and discussed here. These kinds of cases are “controversial” almost by definition, because no one will see enough patients with the same rare condition to study it systematically. Thus there may not be much scientific literature on the patient’s condition, and the surgeon must provide treatment based on clinical experience and analogy to more common conditions. The rarity of the patient’s condition does not necessarily mean that they are more difficult to treat or less likely to benefit from treatment. So fusion surgery should be considered medically appropriate, if established non- operative treatments have been unsuccessful.
At the same time, the spine community should strive to continuously improve the quality of care received by patients with rare or unusual conditions. The best way to do this is to pool experience on a global level. Professional societies play a key role here in two ways. First, the professional society serves as the medium through which the treating surgeon can find a colleague somewhere else in the world who had experience with a similar case and can confer about it. Second, the professional society encourages proper study and reporting on rare and unusual cases, so surgeons can learn from their colleagues’ past experiences, rather than having to reinvent the wheel each time such a case appears. So treatment should be provided only after conferring with a professional society and agreeing to report on the case, if the patient consents.
16. Degenerative Disk Disease in the Elderly.
Pure DDD without other co-diagnoses is rather rare in patients over age 65. These patients usually have other co-diagnoses, such as degenerative spondylolisthesis or degenerative scoliosis, in which case their treatment indications are discussed above under those indications. Lumbar spinal fusion for pure DDD is presumably medically appropriate in the elderly but remains poorly studied in this population,[Schafer] because of its relative rarity. The fundamental scientific basis for performing lumbar fusion for DDD is the 6 randomized comparative trials that have been systematically reviewed, as discussed above.[Blumenthal; Brox 2003; Brox 2006; Fairbank; Fritzell; Zigler] These 6 studies included patients in the following age ranges: 25-65, 18-55, 25-60, 25-60, 18-60, 18-60. Patients outside these age ranges were excluded by protocol. It cannot be automatically assumed that the results obtained in these studies would apply equally to patients outside these age ranges. So currently there is a shortage of evidence supporting fusion for DDD in patients over age 65.[Schafer] Lumbar fusion is performed in the elderly mainly on the basis of presumed analogy to middle-age patients.
The problem though is that disk degeneration increases with age,[Adams; Haefeli; Miller; Powell] and asymptomatic degenerated disks occur quite frequently in the elderly population [Deyo; Powell] Thus for example, among 70 year-olds, 80% of disks are abnormal [Powell] and 60% show severe degeneration [Urban]. So as a person ages, it becomes increasingly difficult to assume a relationship between degenerative findings on imaging and clinical symptoms, because on the one hand asymptomatic degeneration is prevalent in the elderly population and on the other hand elderly patients are more likely to show degeneration at multiple levels, making it difficult to know which one(s) are the source of pain.[Powell]
Additionally, comorbidities or lower general health status may be more common in elderly patients, making anesthesia, operation, and recovery all more difficult. Thus there may be a high risk of complications or poor outcomes in elderly patients.[Cloyd]
Despite these reservations, there is also no evidence suggesting that properly selected elderly patients with DDD would not benefit from lumbar fusion surgery as much as adults in mid-life. Without such evidence, it is questionable to deny treatment to a patient merely on the basis of his or her age. The available clinical studies are of lower quality, but they do not provide a basis for denying lumbar fusion to elderly patients. For example, one small retrospective study on circumferential multilevel fusion for DDD found no differences between elderly and mid-life patients, with very substantial improvements in pain yet clinically minimal improvement in disability in both groups.[Acosta] Insufficient evidence of benefit should not be misconstrued as evidence of insufficient benefit.
More research is needed on lumbar fusion for DDD in the elderly. Until then, single-level lumbar fusion for DDD should be considered medically appropriate in elderly patients meeting all the selection criteria listed above for adults. If possible and if the patient consents, clinical data should be collected, either in the framework of a research study or for submission to a patient registry, with the intent of analyzing the effect of age on clinical outcomes.
References: Acosta; Adams; Blumenthal; Brox 2003; Brox 2006; Cloyd; Deyo; Fairbank; Fritzell; Haefeli; Miller; Powell; Schafer; Urban; Zigler
17. Degenerative Disk Disease at Multiple Levels.
Lumbar spinal fusion at more than 2 levels for pure DDD in the absence of other diagnoses remains poorly studied. The fundamental scientific basis for performing lumbar fusion for DDD is the 6 randomized comparative trials that have been systematically review, as discussed above. Two of these studies had no patients operated at more than one level,[Blumenthal; Zigler] three other studies had no patients operated at more than two levels,[Brox 2003; Brox 2006; Fritzell] and one study had 70 patients fused at more than one level, but did not specify how many, if any, were fused at more than 2 levels or whether their outcomes were comparable.[Fairbank]
Only a few studies report on fusion at 3 or more levels for DDD. One retrospective study showed that DDD patients fused at 3-5 levels had almost as much improvement of health-related quality-of-life (SF-36) as patients fused at only 1-2 levels.[Lettice] But the multilevel patients had noticeably higher rates of complications, pseudoarthrosis, and reoperation. The authors emphasized the importance of proper patient selection, including pressure-controlled diskography, and demonstrated patient commitment to recovery through participation in a preoperative aquatic conditioning program. Another recent retrospective study reported on circumferential fusion at a mean (range) of 4 (3-8) levels for DDD in 80 patients.[Suratwala] Mean ODI improved from 50 at pre- op to 35 at follow-up (2-7 years post-op) in the 69 patients with both data points, which is a clinically meaningful amount of improvement. The repeat surgery rate was 34% during the entire follow-up period. Return to work was 75%. One major limitation to this study though is that the outcome data was based upon a questionnaire mailed to 125 patients, of whom only 80 responded. Non-responders (36%) may have refused to return the postal questionnaire because of worse outcomes and/or dissatisfaction, thereby substantially skewing the results reported. A third retrospective study reported on circumferential fusion at a minimum of 2 levels and mean of about 3.4 levels for DDD in mid-life and elderly patients.[Acosta] At short-term follow-up, they reported very substantial improvements in VAS pain score but minimal change in ODI scores. Together, these three level III studies show that fusion at 3 levels for DDD appears promising and merits further, better-designed clinical research.
Disk degeneration is seen mostly at L4/L5 and L5/S1; at the other 3 lumbar levels, DDD is uncommon. This might suggest that patients presenting with degeneration at 3 or more levels are somehow different from most DDD patients – perhaps more genetically prone to disk degeneration.
If loss of motion is a risk factor for accelerating disk degeneration at adjacent levels, then the more levels fused, the greater the risk.[Levin]
If signs of degeneration are present at more than two levels on imaging, the surgeon should consider that perhaps only one or two of these degenerated discs are actually the “pain generator” and that fusion at one or two levels may be sufficient to relieve the patient’s pain and disability, despite imaging signs of degeneration at other levels. Provocative diskography can usually help make this diagnostic distinction.
At the present time, there is insufficient evidence to support performing fusion at more than 2 levels for DDD (or more than 1 level in patients over age 65). Retrospective publication of available data on multilevel fusions would be helpful to quickly know more about the outcomes from current practice. The evidence currently available supports the initiation of prospective comparative trials on 3-level fusions for DDD. Three-level fusion for DDD may be considered a medically appropriate, investigational treatment option in the framework of a well-designed, prospective multicenter comparative trial. Three-level fusions for DDD should only be performed in the framework of such research studies or when indicated on a case by case basis after peer review. Four and five level fusions for DDD should not be performed at this time until after studies have clearly established that three-level fusions for DDD are medically appropriate.
References: Acosta; Blumenthal; Brox 2003; Brox 2006; Fairbank; Fritzell; Lettice; Levin; Suratwala; Zigler
18. Facet Syndrome.
The facet joints play an important biomechanical role in spinal motion and stability. They sometimes show signs of arthritic inflammation or cartilage necrosis, similar to what is seen in other synovial joints.[Eisenstein] Low back pain may be temporarily relieved by injection of anesthetics into the facet joints. Therefore it is was previously believed that the facet joints are a source of pain, and fusing them might bring relief.[Eisenstein]
This opinion is no longer generally accepted. In 1992, a set of three studies concluded that the facet joint is not a major source of low back pain, and facet blocks are no more effective than placebo and do not prognosticate response to fusion.[Jackson] A narrative review paper in 1993 wrote, “The validity of the commonly used diagnosis of facet syndrome is now being questioned, and a favorable response to injection of the facet joints should not be considered an indication for posterior lumbar fusion.”[Tsang] Similarly, in 1995, a review of the scant literature on facet joint syndrome concluded that “no established criteria exist for lumbar fusion based on facet joint syndrome.”[Zdeblick] One prospective study did report excellent or good outcomes in 98 (84%) of 119 patients treated surgically for facet syndrome.[Markwalder] However, many of the patients had other co-diagnoses, including disk herniation or degenerated disks, and some of the patients were treated with Graf stabilization instead of fusion. Most problematic, the only clinical outcome reported was a semi-quantitative evaluation of work status and pain (“excellent, good, satisfactory, moderate, poor”) at post-op only, which makes it difficult to know how much improvement was really obtained. Aside from this severely limited study, it seems that no further noteworthy clinical reports on facet syndrome have appeared since the mid-1990s.
Thus lumbar fusion should not be performed for “facet syndrome” outside the framework of a well-designed prospective comparative trial. The pre-requisites for any such trial are: 1) better evidence that the facet joints alone can be the source of back pain, and 2) greater consensus on a diagnostic definition of “facet syndrome”. In some cases of severe facet degeneration, the patient may be indicated for fusion on the basis of spondylolisthesis or other local deformity, but then the indication for fusion is “spondylolisthesis” or “deformity”, as discussed above, not “facet syndrome”.
References: Eisenstein; Jackson; Markwalder; Tsang; Zdeblick
19. Stenosis (as defined above). Stenosis in the absence of spondylolisthesis or spinal instability can be treated adequately by decompression alone. Nothing is gained by adding a fusion in these cases.
References: Resnick pt 10; Sengupta; Weinstein; White
20. Initial Disk Herniation. Initial disk herniation should be treated by microdiskectomy alone, if conservative medical management has been inadequate. Fusion is not necessary. There is insufficient evidence to suggest any benefit of performing a fusion for initial disk herniation.
References: Herkowitz; Moschetti; Resnick pt 8
21. Chronic Low Back Pain without Any Clear Cause on Imaging. Non-specific low back pain without an identifiable cause on imaging should be treated by conservative medical management. If the pain persists without any spinal explanation, the patient should be referred for neurologic or psychiatric evaluation. Intensive multidisciplinary rehabilitation may also be beneficial for these patients. Lumbar fusion is not warranted for low back pain without a clear etiology demonstrated on imaging.
References: Carragee 2007; Chou 2009a; Heinrich; Zdeblick
Conclusion
Healthcare reform is just getting underway, with many new initiatives to improve the quality of care offered to patients. Medical research continues to report important new findings every day – with easily over 100 new original research papers every month in spine surgery alone. Although lumbar fusion has long been a well-established treatment, our knowledge and experience continues to evolve. The professional societies intend to update this Policy Statement on an annual basis, in light of any new medical evidence and constructive feedback, with the goal of ensuring the best possible treatment to patients with low back problems.
References
Acosta FL, Cloyd JM, Aryan HE, Ames CP. Perioperative complications and clinical outcomes of multilevel circumferential lumbar spinal fusion in the elderly. J Clin Neurosci. 2009; 16: 69 73.
Adams MA, Roughley PJ. What Is Intervertebral Disc Degeneration and What Causes It? Spine. 2006; 31: 2151-2161. Aebi M. The adult scoliosis. Eur Spine J. 2005; 14: 925-948.
Alkherayf F, Wai EK, Tsai EC, Agbi C. Daily smoking and lower back pain in adult Canadians: the Canadian Community Health Survey. J Pain Res. 2010; 3: 155-160.
Allen RT, Rihn JA, Glassman SD, Currier B, Albert TJ, Phillips FM. An Evidence-Based Approach to Spine Surgery. Am J Med Qual. 2009; 24: 15S-24S.
Andersen T, Christensen FB, Langdahl BL, et al. Fusion mass bone quality after uninstrumented spinal fusion in older patients. Eur Spine J. 2010; 19: 2200-2208.
Angevine PD, Deutsch H. Idiopathic Scoliosis. Neurosurgery. 2008; 63: A86-A93.
Berg S, Tullberg T, Branth B, Olerund C, Tropp H. Total disc replacement compared to lumbar fusion: a randomised controlled trial with 2-year follow-up. Eur Spine J. 2009; 18: 1512-1519.
Berven SH, Deviren V, Mitchell B, Wahba G, Hu SS, Bradford DS. Operative Management of Degenerative Scoliosis: An Evidence-Based Approach to Surgical Strategies Based on Clinical and Radiographic Outcomes. Neurosurg Clin N Am. 2007; 18: 261-272.
Berven SH, Herkowitz HN. Evidence-Based Medicine for the Spine: Degenerative Spondylolisthesis. Semin Spine Surg. 2009; 21: 238-245.
Birknes JK, White AP, Albert TJ, Shaffrey CI, Harrop JS. Adult Degenerative Scoliosis: A Review. Neurosurgery. 2008; 63: A94- A103.
Bloom BS. Daily regimen and compliance with treatment. BMJ. 2001; 323: 647.
Blumenthal S, McAfee PC, Guyer RD, Hochschuler SH, Geisler FH, Hold RT, Garcia R Jr, Regan JJ, Ohnmeiss DD. A Prospective, Randomized, Multicenter Food and Drug Administration Investigational Device Exemption Study of Lumbar Total Disc ReplacementWith the CHARITÉ Artificial Disc Versus Lumbar Fusion – Part I: Evaluation of Clinical Outcomes. Spine. 2005; 30: 1565-1575.
Bono CM, Lee CK. The Influence of Subdiagnosis on Radiographic and Clinical Outcomes After Lumbar Fusion for Degenerative Disc Disorders: An Analysis of the Literature From Two Decades. Spine. 2005; 30: 227-234.
Boos N, Rieder R, Schade V, et al. The Diagnostic Accuracy of Magnetic Resonance Imaging, Work Perception, and Psychosocial Factors in Identifying Symptomatic Disc Herniations. Spine. 1995; 20: 2613–2625.
Borthakur A, Maurer PM, Fenty M, Wang C, Berger R, Yoder J, Balderston RA, Elliott DM. T1ρ MRI and Discography Pressure as Novel Biomarkers for Disc Degeneration and Low Back Pain. Spine. 2011; online publication ahead of print: DOI 10.1097/BRS.0b013e31820287bf.
Bourghli A, Aunoble S, Le Huec JC. Correlation of clinical outcomes and spinopelvic sagittal alignment after surgical treatment of isthmic spondylolisthesis. Eur Spine J. 2011. [In Press]
Broekmans S, Dobbels F, Milisen K, Morlion B, Vanderschueren S. Medication adherence in patients with chronic non-malignant pain: Is there a problem? Eur J Pain. 2009; 13: 115-123.
Brooks BK, Southam SL, Mlady GW, Logan J, Rosett M. Lumbar spine spondylolysis in the adult population: using computed tomography to evaluate the possibility of adult onset lumbar spondylosis as a cause of back pain. Skeletal Radiol. 2010; 39: 669- 673.
Brown CW, Orme TJ, Richardson HD. The Rate of Pseudarthrosis (Surgical Nonunion) in Patients Who Are Smokers and Patients Who Are Nonsmokers: A Comparison Study. Spine. 1986; 11: 942-943.
Brox JI, Nygaard ØP, Holm I, Keller A, Ingebrigtsen T, Reikerås O. Four-year follow-up of surgical versus non-surgical therapy for chronic low back pain. Ann Rheum Dis. 2010; 69: 16431648.
Brox JI, Reikerås O, Nygaard Ø, et al. Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: A prospective randomized controlled study. Pain. 2006; 122: 145-155.
Brox JI, Sorensen R, Friis A, et al. Randomized Clinical Trial of Lumbar Instrumented Fusion and Cognitive Intervention and Exercises in Patients with Chronic Low Back Pain and Disc Degeneration. Spine. 2003; 28: 1913-1921.
Burkus JK, Gornet MF, Schuler TC, Kleeman TJ, Zdeblick TA. Six-Year Outcomes of Anterior Lumbar Interbody Arthodesis with Use of Interbody Fusion Cages and Recombinant Human Bone Morphogenic Protein-2. J Bone Joint Surg Am. 2009; 91: 1181- 1189.
Carragee EJ. The role of surgery in low back pain. Curr Orthop. 2007; 21: 9-16.
Carragee EJ, Don AS, Hurwitz EL, Cuellar JM, Carrino JA, Herzog R. Does Discography Cause Accelerated Progression of Degeneration Changes in the Lumbar Disc: A Ten-Year Matched Cohort Study. Spine. 2009; 34: 2338-2345.
Chou R, Baisden J, Carragee EJ, Resnick DK, Shaffer WO, Loeser JD. Surgery for Low Back Pain: A Review of the Evidence for an American Pain Society Clinical Practice Guideline. Spine. 2009b; 34: 1094-1109.
Chou R, Loeser JD, Owens DK, et al. Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain: An Evidence-Based Clinical Practice Guideline From the American Pain Society. Spine. 2009a; 34: 1066-1077.
Cloyd JM, Acosta FL Jr, Ames CP. Complications and outcomes of lumbar spine surgery in elderly people: a review of the literature. J Am Geriatr Soc. 2008; 56: 1318-1327.
Coe M, Mirza S, Sengupta D. The Role of Fusion for Discogenic Axial Back Pain Without Associated Leg Pain, Spondylolisthesis or Stenosis: An Evidence-Based Review. Semin Spine Surg. 2009; 21: 246-256.
Cohen SP, Larkin TM, Barna SA, Palmer WE, Hecht AC, Stojanovic MP. Lumbar Discography: A Comprehensive Review of Outcome Studies, Diagnostic Accuracy, and Principles. Reg Anesth Pain Med. 2005; 30: 163-183.
Colhoun E, McCall IW, Williams L, Cassar Pullicino VN. Provocation Discography as a Guide to Planning Operations on the Spine. JBJS. 1988; 70-B: 267-271.
Daftari TK, Whitesides TE Jr, Heller JG, Goodrich AC, McCarey BE, Hutton WC. Nicotine on the Revascularization of Bone Graft: An Experimental Study in Rabbits. Spine. 1994; 19: 904-911.
Das SK. Harmful health effects of cigarette smoking. Mol Cell Biochem. 2003; 253: 159-165.
Daubs M, Patel A, Willick S, Richard K, Hansen P, Petron D, Brodke DS. Clinical Instinct vs. Standardized Questionnaire: The Spine Specialists Ability to Detect Psychological Distress. Spine J. 2008; 8: 1S.
DeBerard MS, Masters KS, Colledge AL, Schleusener RL, Schlegel JD. Outcomes of Posterolateral Lumbar Fusion in Utah Patients Receiving Workers’ Compensation: A Retrospective Cohort Study. Spine. 2001; 26: 738-747.
Delamarter R, Zigler JE, Balderston RA, Cammisa FP, Goldstein JA, Spivak JM. Prospective, Randomized, Multicenter Food and Drug Administration Investigational Device Exemption Study of the ProDisc-L Total Disc Replacement Compared with Circumferential Arthrodesis for the Treatment of Two-Level Lumbar Degenerative Disc Disease: Results at Twenty-four Months. J Bone Joint Surg Am. 2011; 93: 1-11.
Deyo RA, Phillips WR. Low Back Pain: A Primary Care Challenge. Spine. 1996; 21: 28262832.
Eisenstein SM, Parry CR. The Lumbar Facet Arthrosis Syndrome: Clinical Presentation and Articular Surface Changes. JBJS. 1987; 69-B: 3-7.
Errico TJ. The Role of Diskography in the 1980s. Radiology. 1987; 162: 285-286.
Evans L, Spelman M. The Problem of Non-compliance with Drug Therapy. Drugs. 1983; 25: 63-76.
Fairbank J, Frost H, Wilson-MacDonald J, Yu L-M, Barker K, Collins R, the Spine Stabilisation Trial Group. Randomised controlled trial to compare surgical stabilization of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: the MRC spine stabilization trial. BMJ. 2005; 330: 1233.
Farcy J-PC, Schwab FJ. Management of Flatback and Related Kyphotic Decompensation Syndromes. Spine. 1997; 22: 2452-2457.
Florence DW, Miller TC. Functional overlay in work-related injury: A system for differentiating conscious from subconscious motivation of persisting symptoms. Postgrad Med. 1985; 77: 97- 105.
Fritzell P, Hägg O, Wessberg P, Nordwall A, the Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: Lumbar Fusion Versus Nonsurgical Treatment for Chronic Low Back Pain: A Multicenter Randomized Controlled Trial From the Swedish Lumbar Spine Study Group. Spine. 2001; 26: 2521-2534.
Gold DT, McClung B. Approaches to Patient Education: Emphasizing the Long-Term Value of Compliance and Persistence. Am J Med. 2006; 119: S32-S37.
Goldman LS, Nielsen NH, Champion HC, for the Council on Scientific Affairs of the American Medical Association. J Gen Intern Med. 1999; 14: 569-580.
Gonzales JJ, Magruder KM, Keith SJ. Mental Disorders in Primary Care Services: An Update. Public Health Rep. 1994; 109: 251- 258.
Guyer RD, McAfee PC, Banco RJ, et al. Prospective, randomized multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with theCHARITÉ artificial disc versus lumbar fusion: Five-year follow-up. Spine J. 2009; 9: 374-386.
Guzmán J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombadier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001; 322: 1511-1516.
Haefeli M, Kalberer F, Saegesser D, Nerlich AG, Boos N, Paesold G. The Course of Macroscopic Degeneration in the Human Lumbar Intervertebral Disc. Spine. 2006; 31: 15221531.
Heinrich TW. Medical Unexplained Symptoms and the Concept of Somatization. WI Med J. 2004; 103: 83-87.
Herkowitz HN, Sidhu KS. Lumbar Spine Fusion in the Treatment of Degenerative Conditions: Current Indications and Recommendations. J Am Acad Orthop Surg. 1995; 3: 123-135.
Heuch I, Hagen K, Heuch I, Nygaard Ø, Zwart J-A. The Impact of Body Mass Index on the Prevalence of Low Back Pain: The HUNT Study. Spine. 2010; 35: 764-768.
Hopp E, Tsou PM. Postdecompression Lumbar Instability. Clin Orthop Relat Res. 1988; 227: 143–151.
Jack K, McLean SM, Moffet JK, Gerdiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man Ther. 2010; 15: 220-228.
Jackson RP. The Facet Syndrome: Myth or Reality? Clin Orthop Relat Res. 1992; 279: 110-21.
Jacobs WCH, Vreeling A, De Kleuver M. Fusion for low-grade adult isthmic spondylolisthesis: a systematic review of the literature. Eur Spine J. 2006; 15: 391-402.
Kalichman L, Kim DH, Li L, Guermazi A, Berkin V, Hunter DJ. Spondylolysis and Spondylolisthesis: Prevalence and Association With Low Back Pain in the Adult Community-Based Population. Spine. 2009; 34: 199-205.
Klein G, Mehlman CT, McCarthy M. Nonoperative Treatment of Spondylolysis and Grade I Spondylolisthesis in Children and Young Adults: A Meta-analysis of Observational Studies. J Pediatr Orthop. 2009; 29: 146-156.
Knaub MA, Won DS, MCGuire R, Herkowitz HN. Lumbar Spinal Stenosis: Indications for Arthrodesis and Spinal Instrumentation. Instr Course Lect. 2005; 54: 313-319.
Kornbluth ID, Freedman MK, Holding MY, Overton EA, Saulino MF. Interventions in Chronic Pain Management: 4 – Monitoring Progress and Compliance in Chronic Pain Management. Arch Phys Med Rehabil. 2008; 89: S51-S55.
Kurd MF, Patel D, Norton R, Picetti G, Friel B, Vaccaro AR. Nonoperative Treatment of Symptomatic Spondylolysis. J Spinal Disord Tech. 2007; 20: 560-564.
LaCaille RA, DeBerard MS, LaCaille LJ, Masters KS, Colledge AL. Obesity and litigation predict workers’ compensation costs associated with interbody cage lumbar fusion. Spine J. 2007; 7: 266-272.
LaCaille RA, DeBerard MS, Masters KS, Colledge AL, Bacon W. Presurgical biopsychosocial factors predict multidimensional patient outcomes of interbody cage lumbar fusion. Spine J. 2005; 5: 71-78.
Lagrone MO, Bradford DS, Moe JH, Lonstein JE, Winter RB, Ogilvie JW. Treatment of Symptomatic Flatback after Spinal Fusion. JBone Joint Surg Am. 1988; 70: 569-580.
Leboeuf-Yde C, Kyvik KO, Brunn NH. Low Back Pain and Lifestyle: Part II – Obesity: Information From a Population-based Sample of 29,424 Twin Subjects. Spine. 1999; 24: 779 -784.
Lee C, Dorcil J, Radomisli TE. Nonunion of the Spine: A Review. Clin Orthop. 2004; 419: 71-75.
Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998; 7: 99-103.
Le Huec JC, Aunoble S, Rigal J. Pelvic parameters: origin and significance. Eur Spine J. [In Press]
Lemelin J, Hotz S, Swensen R, Elmslie T. Depression in primary care: Why do we miss the diagnosis? Can Fam Physician. 1994; 40: 104-108.
Lettice JJ, Kula TA, Derby R, Kim BJ, Lee SH, Seo KS. Does the Number of Levels Affect Lumbar Fusion Outcome? Spine. 2005; 30: 675-681.
Levin DA, Hale JJ, Bendo JA. Adjacent Segment Degeneration Following Spinal Fusion for Degenerative Disc Disease. Bull NYU Hosp Jt Dis. 2007; 65: 29-36.
Lim MR, Yoon SC, Green DW. Symptomatic spondylolysis: diagnosis and treatment. Curr Opin Pediatr. 2004; 16: 37-46. Lonstein JE. Scoliosis: Surgical versus Nonsurgical Treatment. Clin Orthop Relat Res. 2006; 443: 248-259.
Lyznicki JM, Young DC, Riggs JA, Davis RM, for the Council on Scientific Affairs of the American Medical Association. Obesity: Assessment and Management in Primary Care. Am Fam Physician. 2001; 63: 2185-2196.
Mac-Thiong JM, Roussouly P, Berthonnaud E, Guigui P. Sagittal Parameters of Global Spinal Balance: Normative Values from a Prospective Cohort of Seven Hundred Nine Caucasian Asymptomatic Adults. Spine. 2010; 35: E1193-E1198.
Markwalder TM, Mérat M. The Lumbar and Lumbosacral Facet-Syndrome: Diagnostic Measures, Surgical Treatment and Results in 119 Patients. Acta Neurochir. 1994; 128: 40-46.
Martin CR, Gruszczynski AT, Braunsfurth HA, Fallatah SM, O’Neil J, Wai EK. The Surgical Management of Degenerative Lumbar Spondylolisthesis: A Systematic Review. Spine. 2007; 32: 1791-1798.
McIvor A, Kayser J, Assaad J-M, Brosky G, DemarestP, Desmarais P, Hampson C, Khara M, Pathammavong R, Weinberg R. Best practices for smoking cessation interventions in primary care. Can Respir J. 2009; 16: 129-134.
Metz LM, Deviren V. Low-Grade Spondylolisthesis. Neurosurg Clin N Am. 2007; 18: 237-248.
Møller A, Tønnesen H. Risk reduction: Perioperative smoking intervention. Best Pract Res Clin Anaesthesiol. 2006; 20: 237-248.
Moschetti W, Pearson AM, Abdu WA. Treatment of Disc Herniation: An Evidence-Based Review. Semin Spine Surg. 2009; 21: 223-229.
Nejat EJ, Polotsky AJ, Pal L. Predictors of chronic disease at midlife and beyond -the health risks of obesity. Maturitas. 2010; 65: 106-111.
Oskouian RJ, Schaffrey CI. Degenerative Lumbar Scoliosis. Neurosurg Clin N Am. 2006; 17: 299-315.
Österman H, Sund R, Seitsalo S, Keskimäki I. Risk of Multiple Reoperations After Lumbar Discectomy: A Population-Based Study. Spine. 2003; 28: 621-627.
Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent Segment Disease after Lumbar or Lumbosacral Fusion: Review of the Literature. Spine. 2004; 29: 1938-1944.
Patel N, Bagan B, Vadera S, Maltenfort MG, Deutsch H, Vaccaro AR, Harrop J, Sharan A, Ratliff JK. Obesity and spine surgery: relation to perioperative complications. J Neurosurg Spine. 2007; 6: 291-297.
Pellet N, Aunoble S, Meyrat R, Rigal J, Le Huec JC. Sagittal balance parameters influence indications for lumbar disc arthroplasty or ALIF. Eur Spine J. [In Press]
Powell MC, Wilson M, Szypryt P, Symonds EM, Worthington BS. Prevalence of lumbar disc degeneration observed by magnetic resonance in symptomless women. Lancet. 1986; 2(8520): 1366-1367.
Pritchett JW, Bortel DT. Degenerative Symptomatic Lumbar Scoliosis. Spine. 1993; 18: 700-703.
Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine – Part 6: magnetic resonance imaging and discography for patient selection for lumbar fusion. J Neurosurg Spine. 2005; 2: 662-669.
Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine – Part 8: lumbar fusion for disc herniation and radiculopathy. J Neurosurg Spine. 2005; 2: 673-678.
Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine – Part 9: fusion in patients with stenosis and spondylolisthesis. J Neurosurg Spine. 2005; 2: 679-685.
Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine – Part 10: fusion following decompression in patients with stenosis without spondylolisthesis. J Neurosurg Spine. 2005; 2: 686-691.
Rosenow EC III. Patients’ Understanding of and Compliance With Medications: The Sixth Vital Sign? Mayo Clin Proc. 2005; 80: 983-987.
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the Normal Variation in the Sagittal Alignment of the Human Lumbar Spine and Pelvis in the Standing Position. Spine. 2005; 30: 346-353.
Sanmartin C, Murphy K, Choptain N, et al. Appropriateness of healthcare interventions: Concepts and scoping of the published literature. Int J Technol Assess Health Care. 2008; 24: 342-349.
Sansur CA, Reames DL, Smith JS, et al. Morbidity and mortality in the surgical treatment of 10,242 adults with spondylolisthesis. J Neurosurg Spine. 2010; 13: 589-593.
Sasso RC, Foulk DM, Hahn M. Prospective, Randomized Trial of Metal-on-Metal Artificial Lumbar Disc Replacement. Spine. 2008; 33: 123-131.
Sasso RC, Kitchel SH, Dawson EG. A Prospective, Randomized Controlled Clinical Trial of Anterior Lumbar Interbody Fusion Using a Titanium Cylindrical Threaded Fusion Device. Spine. 2004; 29: 113-122.
Schafer J, O’Connor D, Feinglass S, Salive M. Medicare Evidence Development and Coverage Advisory Committee Meeting on Lumbar Fusion Surgery for Treatment of Chronic Back Pain From Degenerative Disc Disease. Spine. 2007; 32: 2403-2404.
Schwab F, Farcy J-P, Bridwell K, Berven S, Glassman S, Harrast J, Horton W. A Clinical Impact Classificaiton of Scoliosis in the Adult. Spine. 2006; 31: 2109-2114.
Schwab F, Patel A, Ungar B, Farcy J-P, Lafage V. Adult Spinal Deformity – Postoperative Standing Imbalance: How Much Can You Tolerate? An Overview of Key Parameters in Assessing Alignment and Planning Corrective Surgery. Spine. 2010; 35: 2224- 2231.
Sengupta DK, Herkowitz HN. Lumbar spinal stenosis: Treatment strategies and indications for surgery. Orthop Clin N Am. 2003; 34: 281-295.
Shamji MF, Parker S, Cook C, Pietrobon R, Brown C, Isaacs RE. Impact of Body Habitus on Perioperative Morbidity Associated With Fusion of the Thoracolumbar and Lumbar Spine. Neurosurgery. 2009; 65: 490-498.
Sherman CB. Health Effects of Cigarette Smoking. Clin Chest Med. 1991; 12: 643-658.
Silva FE, Lenke LG. Adult degenerative scoliosis: evaluation and management. Neurosurg Focus. 2010; 28: E1.
Smith HS. Smoking-Induced Nociception. Pain Physician. 2011; 14: E1-E4.
Strömqvist B, Fritzell P, Hägg O, Jönsson B. One-year report from the Swedish National Spine Register. Acta Orthop Scand. 2001; 72: 99-106.
Suratwala SJ, Pinto MR, Gilbert TJ, Winter RB, Wroblewski JM. Functional and Radiological Outcomes of 360 Degrees Fusion of Three or More Motion Levels in the Lumbar Spine for Degenerative Disc Disease. Spine. 2009; 34: E351-358.
Sutherland G. Smoking: can we really make a difference. Heart. 2003; 89: ii25-ii27.
Swartz KR, Trost GR. Recurrent lumbar disc herniation. Neurosurg Focus. 2003; 15: 10.
Tsang IKY. Perspective on low back pain. Curr Opin Rheumatol. 1993; 5: 219-223.
Urban JPG, Roberts S. Degeneration of the intervertebral disc. Arthritis Res Ther. 2003; 5: 120-130.
Vogt MT, Hanscom B, Lauerman WC, Kang JD. Influence of Smoking on the Health Status of Spinal Patients: The National Spine Network Database. Spine. 2002; 27: 313-319.
Wahl C, Gregoire JP, Teo K, Beaulieu M, Labelle S, Leduc B, Cochrane B, Lapointe L, Montague T. Concordance, Compliance and Adherence in Healthcare: Closing Gaps and Improving Outcomes. Healthc Q. 2005; 8: 65-70.
Warner DO. Preoperative Smoking Cessation: The Role of the Primary Care Provider. Mayo Clin Proc. 2005; 80: 252-258.
Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis. NEJM. 2008; 358: 794-810.
White AP, Albert TJ. Evidence-Based Treatment of Lumbar Spinal Stenosis. Semin Spine Surg. 2009; 21: 230-237. Wiggins GC, Ondra SL, Shaffrey CI. Management of iatrogenic flat-back syndrome. Neurosurg Focus. 2003; 15: 8.
Woolf AD, Breedveld F, Kvien TK. Controlling the obesity epidemic is important for maintaining musculoskeletal health. Ann Rheum Dis. 2006; 65: 1401-1402.
Wright EC. Non-compliance–or how many aunts has Matilda? Lancet. 1993; 342: 909-013.
Zdeblick TA. The Treatment of Degenerative Lumbar Disorders. A critical Review of the Literature. Spine. 1995; 20: 126S-137S.
Zigler J, Delamarter R, Spivak JM, et al. Results of the Prospective, Randomized, Multicenter Food and Drug Administration Investigational Device Exemption Study of the ProDisc-L Total Disc Replacement Versus Circumferential Fusion for the Treatment of 1-Level Degenerative Disc Disease. Spine. 2007; 32: 1155-1162.
Zimmermann-Stenzel M, Mannuβ J, Schneider S, Schiltenwolf M. Smoking and Chronic Back Pain: Analyses of the German Telephone Health Survey 2003. Dtsch Arztbl Int. 2008; 105: 441-448.